Early rehabilitation after a stroke. What should patients and families look out for?
Martyna Rydzewska
MSc
Therapy results
What patients say about us

Rehabilitation can only begin once the patient’s condition is considered stable – by which I mean there is no immediate threat to life. The recovery process itself differs depending on whether the stroke was ischaemic or haemorrhagic. There is also a range of other factors that directly influence the therapeutic approach.
Factors that influence the therapeutic approach include the extent of the stroke, the location of the areas of brain damage, psychopathological symptoms, cognitive and memory disorders, hemispatial neglect, aphasia and other speech disorders, heart conditions and the patient’s level of function before the stroke.
Rehabilitation should be started as early as possible!
Some people may imagine that rehabilitation is just exercises with equipment and learning to climb stairs. That, however, is only a fraction of what a professional physiotherapist does with a stroke patient. Patients often ask how their loved one is meant to be rehabilitated when they are lying in bed, barely breathing, unable to move a paralysed arm or leg.
The answer is: there is such a thing as early rehabilitation after a stroke, which prepares the patient for active verticalisation, gait training and coordination and balance exercises.
In the first hours after a stroke, the physiotherapist’s task is to apply kinesiotherapy methods to help prevent pulmonary and thrombotic complications. The patient undergoes therapy designed to prevent respiratory problems and other complications arising from the initial immobility, such as pressure sores, deep vein thrombosis, lymphoedema and joint contractures.
The therapist should also work to restore superficial sensation, using sensorimotor exercises, massage and various sensory stimuli, including thermal ones. All of this depends on the individual needs of the patient and the factors mentioned above.
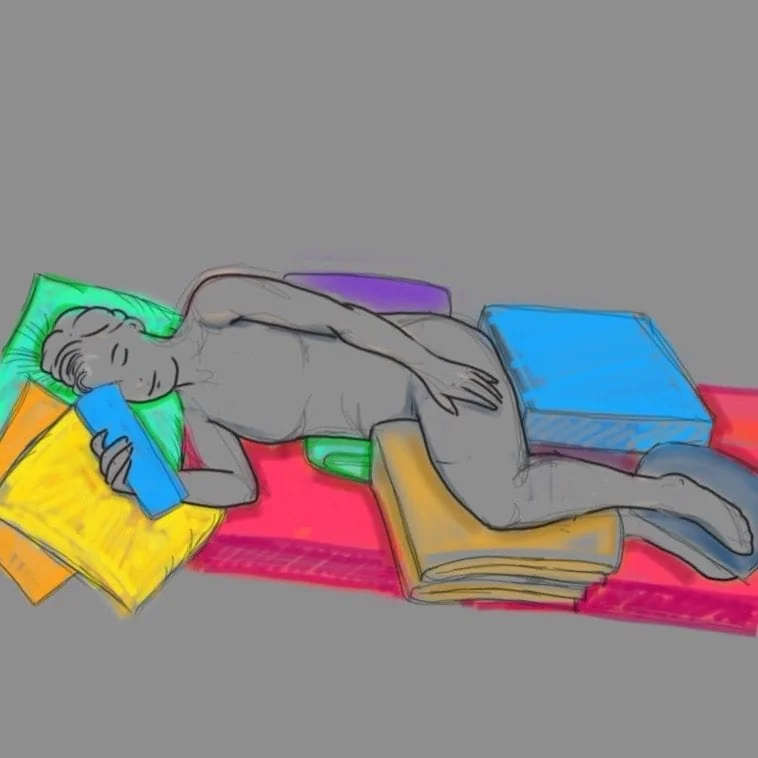
Guidance on positioning the patient in bed
Lying on the back
The upper limb should be set in abduction at the shoulder joint and flexed at the elbow joint at an angle of 90–120 degrees, with the wrist in about 15 degrees of dorsiflexion, a soft roll in the hand, and the thumb extended and abducted. The lower limb should rest in slight abduction and slight internal rotation, with the knee joint slightly bent and the foot set in dorsiflexion.
Rolls, blankets, pillows and towels will help to hold this position. This guidance works well for a patient with flaccid paralysis, whereas with increased muscle tone therapy is needed to normalise tone – for example through transverse mobilisation of the soft tissues.
The patient should be positioned on their sides in bed, including on the side directly affected by paralysis. The return of superficial and deep sensation may be accompanied by persistent pain after a stroke, described as tingling, prickling, burning, tearing or shooting sensations. This is often a good sign, indicating the return of sensation. With properly conducted ongoing neurological rehabilitation, these symptoms subside over time, and function on the affected side can gradually return.
The aim of patient positioning is to stimulate a distribution of muscle tone close to normal, to prevent excessive stretching of certain muscle groups, and to prevent contractures forming in other muscle groups.
Correct positioning of the patient should be carried out around the clock. This is extremely important and prevents abnormal body posture developing in the later stages of rehabilitation.
Kinesiotherapy is meant to stimulate not only the muscular and circulatory systems, but also the nervous system. The latter is highly plastic, so when some cells can no longer perform their function, new substitute nerve connections form. The physiotherapist tries to develop as many of these as possible, and as close as possible to physiological ones.
All of this leads to the initial, partial verticalisation – achieving a sitting position with the legs lowered. These preparations involve stimulating the postural reflex, control of the body’s own axis and movements around that axis. This is why it is important to act quickly and correctly, to prevent new pathological reflexes from forming.
Comprehensive rehabilitation is the key to achieving the best possible outcomes. It must be remembered, however, that individually tailored neurological rehabilitation programmes are a painstaking process, and even the best methods do not always produce quick, spectacular results. Planning the therapy and the active involvement of the patient’s loved ones are essential.
It is important to understand the patient’s needs and to help rather than hinder the therapy. You can hinder it, for example, by showing a lack of understanding towards a patient who needs advice from a psychologist. A patient may have low self-esteem or depression. They should be taught self-care, encouraged towards independence and not helped with everyday tasks unnecessarily, because for the patient these too are a form of therapy.
Progress in this respect is influenced by the involvement of loved ones, a willingness to learn and to understand the patient’s needs, the patient’s condition before the stroke, their ability to learn, their adaptability, their stamina and their social and living circumstances.
Sources
- Kwolek A. Fizjoterapia w neurologii i neurochirurgii, Wydawnictwo Lekarskie PZWL, Warszawa 2012.
- Kwolek A. Rehabilitacja medyczna. Urban&Partner, Wrocław 2003.
- Adamczyk K. Pielęgnowanie chorych po udarach mózgu, Czelej Sp. z o.o., Lublin 2003.
- Kossut M. Wstęp do neuroplastyczności. Neurol. Neurochir. Pol. 2002.
- Malczewski D. Wczesna rehabilitacja i profilaktyka powikłań po udarze mózgu. Terapia 2005.
Read next
Loss of speech after a stroke. Aphasia and the role of the speech therapist in the therapy process.
Aphasia after a stroke is the loss of the ability to understand and produce speech. We explain the types of aphasia, the role of the speech therapist and the directions rehabilitation can take.
Read more →
Can every stroke patient be rehabilitated?
Whether rehabilitation after a stroke is possible depends on the patient’s health, the time since the event and the right choice of therapy. We explain when rehabilitation is possible and how to find the right course of action.
Read more →
When should rehabilitation after a stroke begin?
Early rehabilitation after a stroke usually starts on the neurology ward, but its scope and pace always depend on the patient’s condition and the doctor’s decision.
Read more →
Stroke – brain areas and the effects of brain damage.
The brain is the source of our identity, intellect and emotions. Here is a short guide to the different areas of the brain and the deficits that can arise when they are damaged by an ischaemic stroke.
Read more →
Stroke – emotions, mood and depression
A stroke can damage the brain structures responsible for regulating emotions and mood, which is why depression, anxiety, motivation problems and difficulties with rehabilitation can appear afterwards.
Read more →
Stroke symptoms: how to recognise them and how to respond?
Recognising the symptoms of a stroke quickly and calling for help immediately can save a life and reduce the risk of lasting complications.
Read more →
Spinal cord injury vs spinal cord stroke. What is the difference?
A spinal cord injury and a spinal cord stroke are two distinct conditions with different causes, prognosis and potential deficits. We explain the key differences and the typical consequences of spinal cord damage.
Read more →
10 most common mistakes made by neurological physiotherapists.
Karolina Łozińska describes the most common mistakes made during neurological therapy and the working principles that help to avoid them.
Read more →
Memory loss after a stroke. What it involves and what can help.
Memory loss after a stroke can involve difficulty remembering words, recognising places and learning new things. We explain what can help in everyday functioning and therapy.
Read more →
The next step
Let's talk
We are here to answer any questions you may have about the rehabilitation process.
Describe your case
Send us the details of the patient's condition and we will assess them from a therapeutic perspective.
Email consultation
Write to us describing the condition and the patient's current state of health. We will reply with our view of your situation in the context of rehabilitation.
Video of the patient
You can send us a video showing the patient's current condition. We will respond to your situation and explain the therapeutic options available.