PAJĄK Rehabilitation – SPIDER THERAPY
Specialist therapy for neurological patients — standing upright, balance, trunk control and learning to walk again. A method described in a scientific publication. We are the creators of the PAJĄK device.

PAJĄK rehabilitation, also known as SPIDER Therapy, is a specialised form of therapy used with patients who have neurological conditions and difficulties with standing upright, balance, walking, trunk control and motor coordination.
At the NORMAN Centre, the PAJĄK method is one part of intensive neurological rehabilitation. It is used in particular when a patient needs safe unloading, added loading or precise positioning of the body during exercises.
What is PAJĄK rehabilitation?
PAJĄK is a therapy system built around a special frame and elastic cords that allow the therapist to change how load is placed on the patient's body.
This makes it possible to:
- safely support the patient in standing upright,
- partially unload the patient's body weight,
- apply controlled loading to selected parts of the body,
- work on balance,
- stimulate postural reactions,
- work on correct trunk alignment,
- carry out gait training,
- work on limb activity,
- improve control of the centre of gravity.
In practice, PAJĄK does not replace the therapist. It is a tool that allows the physiotherapist to guide the patient's body more precisely and to create the right conditions for active movement.
Why does PAJĄK matter in neurological rehabilitation?
In patients who have suffered damage to the nervous system, the problem is often not simply muscle weakness.
Very often several difficulties occur at the same time:
- balance disorders,
- asymmetrical loading of the limbs,
- difficulty standing upright,
- abnormal muscle tone,
- impaired deep sensation (proprioception),
- difficulty controlling the trunk,
- gait disturbances,
- a fear of moving or of falling.
In such cases, ordinary exercises may not be enough, because the patient is not always able to adopt the correct position, keep their balance or perform a movement safely.
PAJĄK makes it possible to create conditions in which movement becomes easier, safer and more controlled for the patient.
PAJĄK and rehabilitation after a stroke
One of the most important uses of the PAJĄK system is rehabilitation after a stroke.
After a stroke, a patient may have weakness (paresis) down one side of the body, gait disturbances, difficulty maintaining a standing position, problems bearing weight on the limb on the affected side, or impaired trunk control.
In such situations, therapy in the PAJĄK can be used to:
- practise standing upright,
- practise transferring body weight,
- activate the weaker, affected side,
- work on pelvic stability,
- improve trunk alignment,
- practise the stance phase of walking,
- control the movement of the lower limb,
- reduce the risk of falling during exercises.
This is especially important for patients who are not yet ready for independent exercises under full body weight.
Therapy video
Results of PAJĄK rehabilitation after a stroke
A patient after an ischaemic stroke — therapy with the PAJĄK device at the NORMAN Centre.

Post-stroke rehabilitation results with the PAJĄK device
Ischaemic stroke — PAJĄK (Spider Therapy) treatment at NORMAN
What does the scientific publication describe?
The scientific publication on the SPIDER/PAJĄK system presented two cases of neurological patients:
- an adult patient after an ischaemic stroke,
- a child with cerebral palsy presenting as hemiparesis (one-sided weakness).
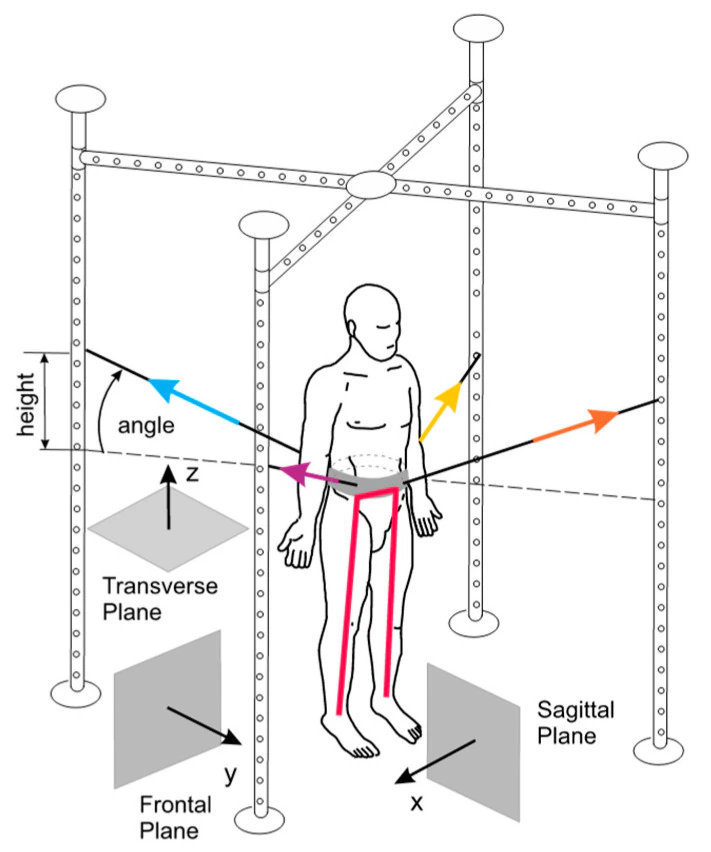
The authors described not only the course of therapy but also proposed a computer model for assessing the forces acting on the patient's body while working in the PAJĄK system.
This matters because, in neurological rehabilitation, observing the patient alone is not always enough. The therapist sees the result of a movement, but cannot always assess precisely which forces are acting on the patient's body and how the load on individual parts of the body changes.
The computer model described in the publication helps to better understand how the arrangement of the cords and expanders affects:
- the patient's centre of gravity,
- the direction in which force is applied,
- the unloading or loading of the limbs,
- body stability,
- the work of the feet,
- postural control.
How does the PAJĄK system work?
The PAJĄK system is based on elastic cords fixed to a special frame and to a belt worn by the patient.
By changing where the cords are attached, the therapist can influence whether the patient's body is:
- unloaded,
- loaded,
- stabilised,
- guided in a particular direction,
- prompted into an active muscular response.
If the attachment point is higher, the system can partially unload the patient. If the attachment point is lower, it can increase the load on a selected segment of the body.
This allows the therapist to match the exercise conditions very precisely to the patient's current abilities.


The stroke patient case described in the publication
The publication describes a 76-year-old patient following an ischaemic stroke affecting the left hemisphere of the brain. The patient had severe right-sided weakness (paresis) and aphasia.
Before rehabilitation began, the patient was unable to stand up unaided. He had considerable difficulty controlling his posture, weakened activity in the trunk muscles and limited ability to move the limb on the affected side on his own.
Therapy using PAJĄK was aimed, among other things, at:
- achieving as active a standing position as possible,
- stimulating balance reactions,
- activating the antigravity muscles,
- gradually loading the limb on the affected side,
- stabilising the pelvis,
- improving control of the knee,
- preparing for gait re-education.
After four weeks of therapy, the patient improved his walking, his ability to move from lying to sitting and from standing to sitting. Before rehabilitation he had been unable to stand up on his own, whereas by the end of therapy he began to move about independently, with someone on hand for safety and using a tripod walking stick.
PAJĄK as support for gait re-education
In rehabilitation after a stroke, one of the hardest stages is the return to safe and, as far as possible, efficient walking.
The challenge is not just taking a step. The patient has to regain control over:
- the trunk,
- the pelvis,
- the lower limb,
- the foot,
- transferring body weight,
- balance,
- protective reactions.
PAJĄK allows the therapist to position the patient's body so that walking exercises are safer and more precise. The demands can be increased gradually, the level of unloading changed, and muscle activity encouraged exactly where the patient's deficit is greatest.
This is why PAJĄK therapy can be an important part of working on gait disorders after a stroke and on restoring lower-limb function.
Therapy video
Rehabilitation with the PAJĄK device — gait re-education
Safe therapy in an upright position — working on walking under controlled conditions.

Rehabilitation with the PAJĄK (Spider Therapy) device
Safe therapy in an upright position — gait re-education
PAJĄK and working on the hand after a stroke
Although PAJĄK is often associated with standing upright and walking, its uses can be broader.
In patients after a stroke, weakness of the hand after a stroke is also a significant problem. The upper limb needs not only strengthening but also improved control, better muscle tone, correct positioning of the shoulder girdle and coordination.
By stabilising the body in the PAJĄK, the therapist can create better conditions for upper-limb exercises, because the patient does not have to spend all their energy simply holding a position.
This is particularly important when problems with the trunk, balance and muscle tone make active work with the hand difficult.
Why must therapy in the PAJĄK be individually tailored?
There is no single, universal PAJĄK therapy protocol that suits every patient.
Every neurological patient is different:
- a different type of weakness (paresis),
- a different level of muscle tone,
- different trunk control,
- a different capacity for standing upright,
- different sensory disturbances,
- a different level of fatigue,
- a different stage of rehabilitation.
That is why the arrangement of the cords, the degree of unloading, the patient's position, the type of exercises and the length of therapy all have to be chosen by an experienced therapist.
PAJĄK offers a great deal, but its effectiveness depends on it being used correctly.
What sets the PAJĄK method apart?
The greatest value of PAJĄK lies in its ability to combine three things:
- Safety.
- Active movement by the patient.
- Precise control over the exercise conditions.
The patient can perform a movement that, without support, would be too difficult or too risky. At the same time, the therapist can gradually reduce the assistance, increase the demands and observe how the patient adapts to the new conditions.
This is what distinguishes PAJĄK from passive suspension. The goal is not merely to hold the patient in position. The goal is active work on function.
PAJĄK at the NORMAN Centre
At the NORMAN Centre, PAJĄK is used as part of comprehensive neurological rehabilitation.
We most often combine it with other forms of therapy, such as:
- neurophysiological therapy,
- gait re-education,
- hand therapy,
- balance exercises,
- trunk therapy,
- work on standing upright,
- functional therapy,
- individual work with a physiotherapist.
PAJĄK is not a separate method detached from everything else. It is a tool that helps us to achieve the goals of rehabilitation more effectively.
Who might PAJĄK rehabilitation be for?
Therapy using the PAJĄK system may be considered for patients with a range of neurological problems, including those:
- after a stroke,
- after a brain injury,
- after surgery for a brain tumour,
- with cerebral palsy,
- with multiple sclerosis,
- with balance disorders,
- with difficulty standing upright,
- with gait disturbances,
- with weakness of the limbs,
- with reduced trunk control.
Eligibility for therapy is always determined by the patient's condition and the assessment of the therapy team.
PAJĄK and the safety of therapy
Patient safety is one of the main reasons for using the PAJĄK system.
A patient who is not yet ready to stand or walk unaided can carry out exercises under controlled conditions. The therapist can reduce the risk of falling, limit compensatory movements and keep better control of the patient's body position.
This is especially important for patients:
- with severe weakness (paresis),
- with balance disorders,
- who are afraid of standing upright,
- with weakened trunk control,
- after a long period of immobilisation,
- after a severe stroke.
What does the scientific publication tell us?
The publication indicates that therapy using the SPIDER/PAJĄK system may support the rehabilitation of neurological patients, particularly when it comes to standing upright, balance, postural control, mobility and gait re-education.
The authors point out that the computer model can help the physiotherapist to better understand the forces acting on the patient's body during therapy. This makes it possible to assess the patient's positioning, the direction of the forces and the changes taking place during rehabilitation more objectively.
At the same time, the publication was preliminary in nature and was based on two case reports. It should therefore not be regarded as definitive proof that the method works for every patient. It is, however, an important piece of work that shows the potential of the PAJĄK system and points the way for further research.
Why does this matter to the patient?
For the patient and their family, what matters most is not the device itself, but whether the therapy helps to restore function.
PAJĄK can be especially valuable when the patient:
- is not yet able to stand unaided,
- is afraid to put weight on the affected side,
- has trouble transferring their body weight,
- loses their balance during exercises,
- needs intensive but safe standing practice,
- needs their body position controlled during movement.
In such situations, PAJĄK makes it possible to start working on function earlier and more safely than under full body weight.
The most important uses of PAJĄK after a stroke
In rehabilitation after a stroke, PAJĄK can be used, among other things, to:
- help the patient stand upright,
- practise loading the affected side,
- re-educate walking,
- work on trunk stability,
- improve balance,
- practise control of the knee,
- work on foot positioning,
- activate the lower limb,
- prepare the patient to move about independently.
This is why PAJĄK therapy can be an important part of comprehensive rehabilitation after a stroke.
The history and development of the method
The PAJĄK/SPIDER system has been used in rehabilitation for many years. The scientific publication notes that the SPIDER system was created in response to a missing link in rehabilitation and has been used with patients suffering from a variety of neurological conditions.
The literature also refers to Norman Łoziński's patent for a sports and rehabilitation device, in particular for patients with disorders of posture and motor activity.
This is an important part of the method's history, because it shows that PAJĄK is not a piece of exercise equipment chosen at random, but a solution developed with patients who have serious impairments of motor function in mind.
Limitations and an honest approach
Every rehabilitation method should be judged sensibly.
PAJĄK can be a very useful tool, but it is not a miracle method that works the same way for every patient. The outcome of therapy depends on many factors:
- the type of injury,
- the time since the illness or injury,
- the degree of weakness (paresis),
- the patient's general condition,
- cognitive ability,
- the patient's cooperation,
- the intensity of therapy,
- the experience of the therapy team.
That is why, at the NORMAN Centre, PAJĄK is part of an individually tailored rehabilitation programme, not an automatic set of exercises.
FAQ
Frequently asked questions about PAJĄK rehabilitation
Is PAJĄK a method for patients after a stroke?
Yes. It can be used with selected patients after a stroke, particularly when there are problems with standing upright, balance, walking, trunk control or loading the affected side.
Does PAJĄK replace conventional rehabilitation?
No. PAJĄK is a tool that supports the therapist's work. It gives the best results as part of a comprehensive neurological rehabilitation programme.
Is therapy in the PAJĄK passive?
It should not be passive. The aim of the therapy is for the patient to work actively on movement, balance, posture and function.
Can PAJĄK help with learning to walk again?
It can support gait re-education, because it allows the therapist to control the loading, the patient's body position and their safety during exercises.
Can every patient exercise in the PAJĄK?
No. The decision is made by the therapy team after assessing the patient's condition. For some patients the therapy can be very helpful, while for others different forms of treatment are more appropriate.
Are there any scientific publications about PAJĄK/SPIDER?
Yes. One of them is the article "SPIDER as A Rehabilitation Tool for Patients with Neurological Disabilities: The Preliminary Research", published in the Journal of Personalized Medicine in 2020.
Source
The content of this page is based on the following publication:
- Sebastian Glowinski, Andrzej Blazejewski, „SPIDER as A Rehabilitation Tool for Patients with Neurological Disabilities: The Preliminary Research”, Journal of Personalized Medicine, 2020, 10(2), 33. DOI: 10.3390/jpm10020033.
- Full text of the publication in PubMed Central (United States National Library of Medicine).
The publication is available Open Access under a Creative Commons Attribution 4.0 licence.
The next step
Let's talk
We are here to answer any questions you may have about the rehabilitation process.
Describe your case
Send us the details of the patient's condition and we will assess them from a therapeutic perspective.
Email consultation
Write to us describing the condition and the patient's current state of health. We will reply with our view of your situation in the context of rehabilitation.
Video of the patient
You can send us a video showing the patient's current condition. We will respond to your situation and explain the therapeutic options available.